

About the author: Ari Allyn-Feuer has a PhD in bioinformatics and is a principal data scientist at a major pharmaceutical company. He develops lifesaving drugs for a living.
Recently we published a framework for thinking about the COVID-19 pandemic, including the six levels of the pandemic from 0 to 5, the three forces that can reduce the virus’s spread (natural immunity, public health measures, and therapies), and the three major possibilities for the long term future of the pandemic. If you haven’t checked that post out yet, it’s a worthy primer before this one.
In this post, we’ll discuss those three scenarios in more depth, including what those scenarios might look like and the forces that will determine which of these three scenarios we end up in.
Scenario 1: Containment and Eradication
This scenario is the most desirable, and until recent weeks it was the one most people were expecting.
We know it’s possible for at least some countries to bring cities and regions back from even a Level 4 epidemic to a state of normality, and that at least some novel coronaviruses (like SARS and MERS) can be eradicated entirely. If every country can do what China has done with its severe outbreak, and track what remains down until the last cases disappear, then the epidemic will end by eradication long before therapies arrive in a global quantity.
How it would happen
While this scenario now looks less likely than ever, it would be a mistake to discount it entirely. The WHO is emphatic that it still remains possible, and there are a number of factors which might help to make this reality.
One, of course, is summer. If the temperature effect proves to be significant, we might be able to spend the summer of 2020 eradicating the disease due to improvements in medical science, rather than letting it slowly spread and then return in fall as the world did with the pandemic flu in the summer of 1918.
We could also ready enough PCR testing capacity to let every country in the world routinely test fever patients, as China and Korea are doing now. However, this would depend on not letting our eye off the ball if the pandemic does abate.
Another is new therapies. While no therapies are likely to be available at global scale in 2020, a number of potential options might be available at smaller scales. For example, some trials of antivirals like protease inhibitors and remdesivir, as well as chloroquine, are now expected to yield results as early as April, and as we’ve discussed, there is the potential for these drugs to be available for hundreds of thousands or perhaps even millions of patients this year.
Regeneron has announced that its anti-SARS-CoV-2 antibody drug, which can be used as both a therapy for diseased patients and a short-acting vaccine, will be available to the tune of 200,000 doses in August. Experimental vaccines based on RNA or proteins may also be shown effective and available in small quantities this year.
While limited quantities of new therapies would be irrelevant if COVID-19 cases continue to escalate out of control, if case numbers can be largely contained, they might be able to help resolve the remaining cases and areas.
What it would look like
Iran, South Korea, and Italy, and the many other countries with emerging clusters that are likely to go to Level 4, would bring their crises under control as China did.
China’s case numbers would continue to dwindle to zero.
Countries around the world would get their testing game together, and over time, fewer new Level 4 clusters would emerge.
The total global burden of COVID-19 would begin to fall, and with the aid of new therapies coming on in small quantities, finally reach zero.
If this happens, the larger hindsight look at the COVID-19 pandemic of 2019-2020 will be that with the aid of scientific and public health advances, the world once again eradicated a novel coronavirus before it got out of hand. With luck, this close brush with global catastrophe would persuade the globe to take a more responsible approach to infectious disease going forward.
Scenario 2: Sideways until Therapies

The second scenario is intermediate. What if most countries manage to do a pretty good job of containing the virus, and prevent the emergence of Level 5 clusters in too many places, but aren’t good enough to reach containment?
For example, what if Italy, Iran, and Korea and other countries resolve their problem as China has, but new Level 4 clusters emerge in that time, and they in turn mostly control it, but by then, other countries have gone Level 4?
What if keeping COVID-19 outbreaks from reaching Level 5 proves a lot easier than pushing them from Level 2 back to Level 0? What if some countries can’t get control of it at all, and go Level 5?
How it would happen
If some countries reach Level 5, the rest of the world will not be able to prevent at least some cases from breaking back into other areas frequently. But if the bulk of the world’s countries do a good enough job controlling case clusters, it may be that parts of the world could go Level 5 while most of the world doesn’t, at least for a while.
This could be aided by the temperature response of the virus, as discussed separately. If the summer offers a meaningful reprieve, it may be possible to use it productively and make preparations that will help every country manage its problems next winter. In addition, some of the poorest areas with the least capacity to respond to a COVID-19 outbreak have warm weather year round.
If the world manages to keep case numbers small relative to the global population and prevent Level 5 from happening in too many places, then over the course of late 2020 and 2021, new therapies arriving in quantity will begin to make the difference.
What it would look like
If the global attack rate of COVID-19 ranged from .1% to 3% in this scenario, it might kill between 150,000 and 7 million people, an event comparable in size to a notable war or natural disaster, but much smaller than the 1918 flu pandemic or the medieval black death.
In this case, the larger look at the COVID-19 pandemic of 2019-2022 will be that with the aid of scientific and public health advances, a pandemic like the 1918 flu was stalled off for long enough that vaccines prevented it from attacking most humans.
Scenario 3: The Big Burn

This is the scenario we’re most worried about, and the one we hope will be avoided at all costs. In this worst-case scenario, a large fraction of humans worldwide wind up getting the virus — it would be a “big burn” comparable to 1918.
How it would happen
We would get a “big burn” if none of the public health measures, treatments, or vaccines we’re trying prove effective enough to get the infection under control in most places in the long run — or if for whatever crazy reasons we don’t commit enough to such measures.
This burn could happen all at once (e.g. if many countries fail to contain their emerging Level 4 clusters, and we get little or no help from the summer heat) or in segments over two or three winters, as was the case with the 1918 pandemic.
What it would look like
If this happened, then most parts of the world would spend several months at Level 5, with many, many sick people and all medical facilities overwhelmed. As in the 1918 flu pandemic, some areas might go to Level 5 more than once. For example, the UK went to Level 5 three times during the 1918 pandemic.
In this case, SARS-CoV-2 would kill tens of millions of people and precipitate a severe global recession. Exactly how many would be a matter of the community attack rate (percentage of humans who got infected), and the case fatality rate.
The National Ebola Training and Education Center published one estimate showing that with 30-40% attack, and .5% CFR, the United States would see about 480,000 deaths and the world about 8 million. This is a responsible estimate of the impact of a “big burn” pandemic from a legitimate authority, even if its CFR estimate is on the lower end of current estimates.
If attack rate were closer to 60%, and the upper end of WHO CFR estimates is borne out, then the USA might see closer to 6 million deaths out of 150 million global deaths. This is the worst-case estimate (unless the CFR of COVID-19 proves to be higher than any current responsible estimates).
An event like this would go down in the history books right next to the 1918 flu pandemic, as simply another iteration of the same event. Just as World War I was once known as simply The Great War, the world will have learned at a great price that an event we thought was unique was just the first of a series, with the length of that series for us to determine.
If a Big Burn happens, how much can we flatten the curve?
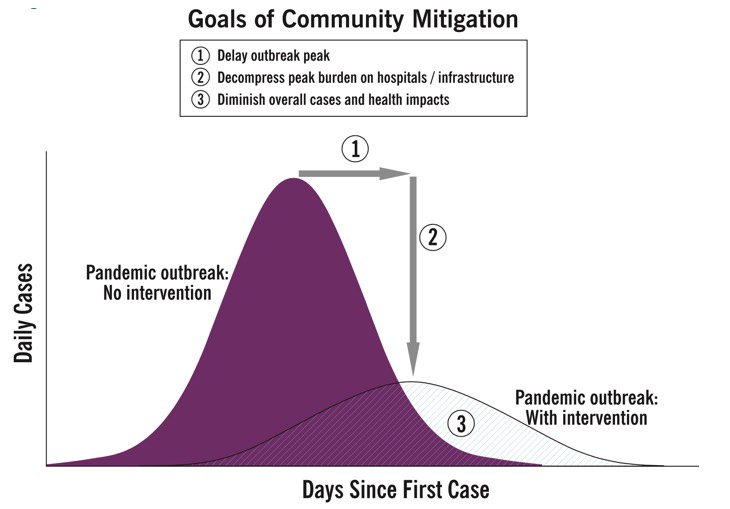
In recent days, social media has been flooded with a discussion of how to “flatten the curve.” The idea is that if a Big Burn happens in a particular area, the people there will be a lot better off the slower it happens, even if the overall attack rate there doesn’t change. The comparison between the experiences of Philadelphia and St. Louis in the United States in the winter of 1918-1919 is a common feature of these discussions.
While this idea is true and important, a lot of messaging has been over-reliant one one particular idea: that the peak rate of cases can be pushed below the capacity of a healthcare system, so that everyone can get good care even if a system hits Level 5 over the long run. This part isn’t really true, as a recent Medium post argued with some heated rhetoric and some math errors, and as a recent Imperial College working paper argued with less of both of these things. The capacity of our healthcare systems is so far below the demands of a Level 5 epidemic that even a slow Level 5 burn will overwhelm hospitals so that most areas see most patients receiving only minimal care.
This may be seen from what’s already happening; there’s a marked difference in CFR between Level 3 and Level 4 areas, because even in Level 4 areas, hospitals are overwhelmed.
The lowest CFRs anywhere are in the area of 1%, and have been seen in areas like Beijing and Yokohama that saw lots of cases but didn’t go Level 4.
Level 4 areas have seen CFRs closer to 3-5%, and a Big Burn would see orders of magnitude more cases at once.
It’s unclear how much worse than this the CFR in a Level 5 area would get, since Level 4 areas are already very overwhelmed. But there’s no real prospect of an area going Level 5 and having a well equipped hospital bed for every critical case. That idea is wholly illusory.
However, it’s worth remembering that even once the false idea about health care system capacity is dispensed with, it’s still absolutely critical to do everything we can to slow the spread of SARS-CoV-2, for a bunch of important reasons:
- This ball game has not been called yet. We may still be able to experience Scenario 1 or Scenario 2 instead of The Big Burn, if we do a good enough job.
- Even if we experience a Big Burn and hospitals are overwhelmed, the less overwhelmed they are, the better.
- Even in an area that experiences a Big Burn, community attack rates can still vary significantly, as they did in 1918, and the differences can mean millions of lives.
No matter what happens, no matter where or when, efforts to reduce spread are still justified. There is no point at which it becomes optimal to let go and stop trying to get the viral coefficient down below one.
What happens after? Can SARS-CoV-2 come back?
After a pandemic, in theory the virus could be eradicated or go endemic (ie. it sticks around like the seasonal flu).
The 1918 pandemic flu largely disappeared, and major outbreaks of that strain have not been seen since. By contrast, the 2009 “Swine Flu” has been seen since, though not in such numbers. The Black Plague even still pokes its head up once in a while, averaging about seven U.S. cases per year.
Whether this happens is obviously of great concern with SARS-CoV-2, since COVID-19 has severity and fatality much higher than endemic respiratory diseases like seasonal flu.
If this happens, a worldwide vaccination campaign with eradication as its goal would be our best bet. Otherwise, it could eventually go pandemic again, or simply kill millions globally every year on an ongoing basis. It’s fairly certain that the vaccine industry can produce a cheap SARS-CoV-2 vaccine on global scale eventually, and if it’s needed, it will be up to the world not to take its eye off the ball.
You are reporting the comment """ by on