

Whether the United States will attain herd immunity against COVID-19 is a hot-button issue right now. Vaccine administration in the United States has fallen by almost 30%, from a peak of about 3.5 million doses a day to about 2.5 million, largely due to flagging demand.
The New York Times surveyed experts and found a consensus that it’s “unlikely” the US will attain herd immunity this year, and various experts have chimed in about what percentage of people vaccinated reaches the herd immunity threshold (HIT).
This is obviously a huge question — reaching herd immunity is the big step needed to get things back to normal. Until we reach HIT, large outbreaks, virus mutations, and economic problems will continue to be at least a threat, and probably a reality.
The press has talked a lot about this risk and why it’s important, but we wanted to add a deeper analysis of what the HIT actually is and how it relates to vaccine penetration.
Summary:
- Contrary to the NY Times piece, the US can achieve herd immunity if we can persuade hesitant adults and vaccinate teens and children.
- But we don’t need to convince or force hardcore antivaxxers — which make up only about 20% of the population — if the people on the fence do the right thing.
- Israel’s COVID-19 infections have plummeted after only vaccinating 60% of the population.
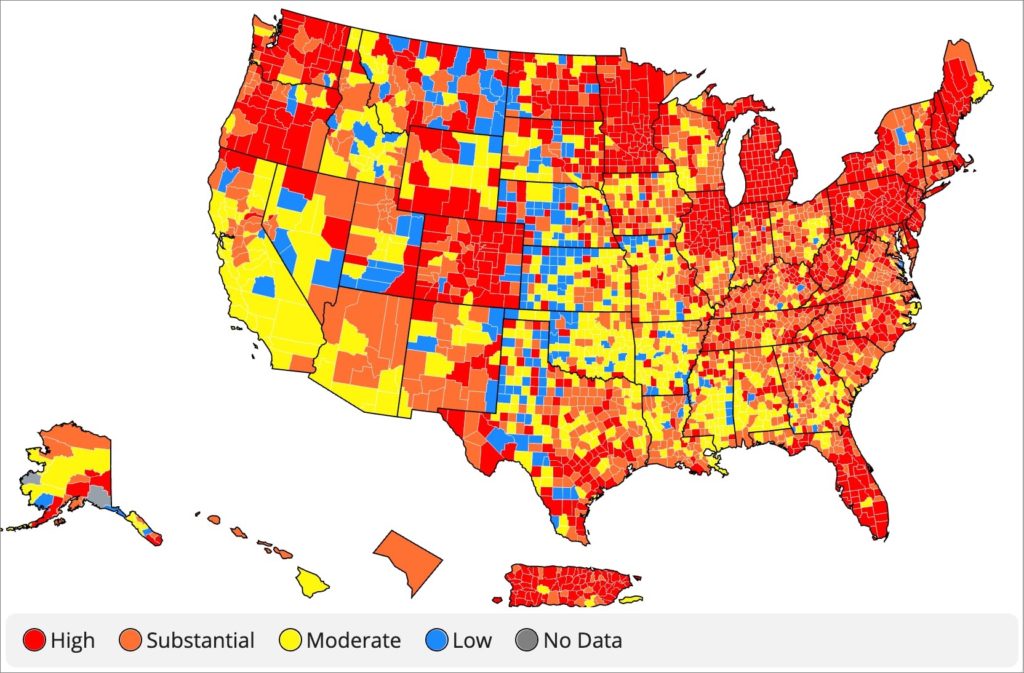
- Anti-vax politics tend to be regional, so there will be some parts of the country that hit herd immunity while others don’t. There may be outbreaks in those anti-vax communities, but it will be limited and burn itself out.
- The higher the percentage of people who are vaccinated, the more likely we can squash scary new mutations with booster shots that are quicker to develop than the original vaccine.

The Herd Immunity Threshold in theory
The herd immunity threshold, stated in terms of the percentage of people who need to be vaccinated, is fuzzy, imprecise, and the subject of controversy. But in a theoretical model, it’s actually mathematically precise, and understanding how experts back out of that precise model to form their opinions about the real world HIT will help us understand what the US has in store, based on our ability to vaccinate people.
In our coverage of the pandemic, we’ve focused heavily on an epidemiological concept called R: the average number of people infected by one person who has COVID-19 (or any disease). In a time or place where R is greater than 1, cases will rise exponentially; where R is less than 1, it will fall exponentially. R0, or “R-nought,” is the value that R adopts in a population where no one has any immunity, and no one is taking any precautions.
For COVID-19, this value is as high as 4 for the wild-type strains, which describes the kind of explosive growth the pandemic experienced in places like Wuhan, Milan, and New York, before people started taking any precautions. For more-transmissible strains like B.1.351 and P.1, R0 may be as high as 5.5.
When stated in terms of the degree of transmission reduction afforded by immunity (including how imperfect that immunity is), and on the assumption that immunity is uniformly distributed and not correlated with contact frequency, the HIT can be precisely stated as 1-1/R0. This is because, with no precautions, R is equal to R0 * (1-I), where I is the percentage of population immunity. When I is equal to 1-1/R0, then R is equal to 1, even with no precautions, and outbreaks cannot grow exponentially. The population has herd immunity. The average infection will give rise to only one other infection (or less), so that the epidemic can no longer grow.
Herd immunity is more complicated in practice
But the real world is more complicated. There are a lot more complicating factors, which account for differing opinions about the degree of vaccination needed for herd immunity in practice.
That’s why, even though politicians have pressed experts like Dr. Fauci to give a specific answer of what percentage of people need to be vaccinated, the experts reply with a more ambiguous range. Fauci, for example, has used wording like “a range around 60-75%.” It’s not politics. It’s just the nature of dealing with too many unknowns, and different experts estimating those unknowns in different ways.
These variances include things that push the HIT in practice both up and down relative to its theoretical value, such as:
- Immunity in the population comes from a number of sources, including several different vaccines and natural immunity, and none of these sources is perfectly effective, nor are they all equally effective. This pushes the HIT up, because we need to vaccinate (or infect) more than 50% of the people to get to 50% population immunity (for example). Countries using lower-efficacy dead-virus vaccines like those from Bharat Biotech, Sinopharm, and Sinovac may be unable to attain herd immunity even by vaccinating 100% of their population.
- Willingness to get vaccinated is not uniform in the population, producing regional and cultural pockets with higher and lower vaccine penetration, compared to the average. This means that higher-vaccination pockets will stop transmission even before the national HIT is achieved as a society-wide average, while lower-vaccination pockets may see ongoing transmission even after it is achieved.
- Contacts are not uniformly distributed, and high contacts (and low precautions) will correlate with preexisting natural immunity, and inversely correlate with willingness to get vaccinated. This pushes the HIT downward, because the people with the most contacts, and those refusing vaccines, will be more likely to have already been infected. Natural immunity will affect a larger portion of the non-vaccinated people, and of interpersonal contacts, than it would if it were randomly distributed.
- The level of public precautions is not going all the way back down to zero any time soon; residual precautions will continue to give us a tailwind to some extent, for a long time. This pushes the HIT downward.
This is why experts are taking such different views of the HIT in practice. Their estimates of R0, and their differing estimates of the impact of all these factors, are leading them to a diversity of opinion.
On the high end, it’s possible to arrive at very, very high values. With the maximal value of R0 for the newest strains at 5.5, the theoretical HIT is 81.8%, a very high figure. With the efficacy of even the best vaccines against transmission at only 90%, and natural immunity at about 80%, in theory it might be necessary to vaccinate nearly 100% of the population to get to the HIT.
But it’s also possible to find support for a lower number, in theory, and especially empirically. The signal example for people who think the HIT is a lot lower in practice is Israel. The small Mediterranean country has vaccinated only about 60% of its population with the highly effective Pfizer vaccine, and has crashed COVID-19 caseloads by 99% in three and a half months despite re-opening nearly everything and largely resuming a normal life.
The HIT in the USA: digging into the real numbers
With all of this in mind, let’s dig into the US’s real situation, asking this question: if the United States manages to convince hesitant people — the ones who tell opinion surveys they are taking a “wait and see” approach — but totally fails to convince anyone who currently says they will not get vaccinated, what lies ahead?
The “no” population differs somewhat by survey, but usually constitutes about 20% of those surveyed. This number has come down from over one-third in surveys taken last fall, but currently seems pretty stable at about 20%.
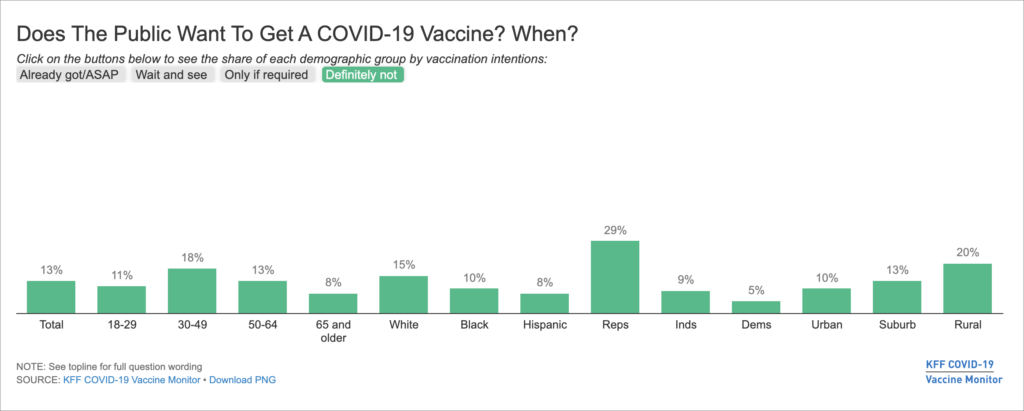
Antivaxxer rates change significantly by state. It’s as low as 7% in places like Massachusetts, which is not only an urban “blue” state but also home to the headquarters of Moderna and a major research facility of Pfizer, leading many residents to feel like COVID-19 vaccines are a hometown cause.
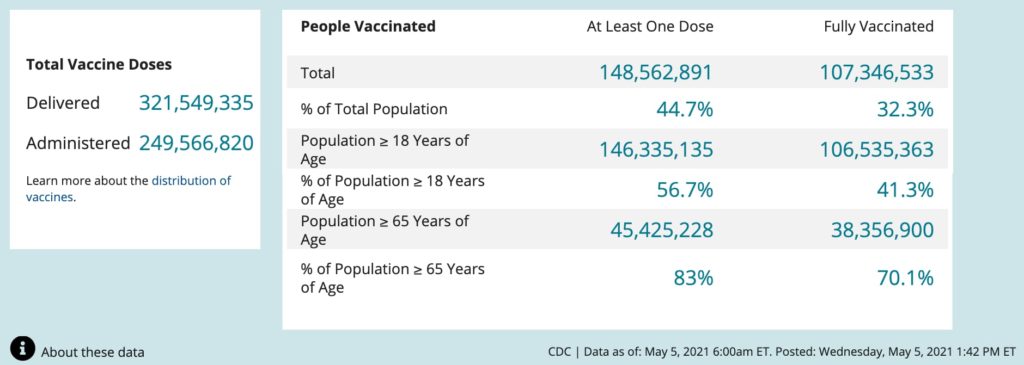
There is every reason to think that the “persuadable” people actually are persuadable and that we can reasonably reach 80% of eligible people vaccinated. We have already vaccinated 83% of Americans over 65 with at least one dose, and hesitancy is not highly correlated with age.
So, if we did manage to vaccinate 80% of eligible people, what would the US immunity level look like?
Now that the FDA has announced it will imminently approve the Pfizer vaccine for children ages 12 and up, 85% of the US population will be eligible for the vaccine. If we get 80% of eligible people vaccinated, that’s 68% of the overall population vaccinated, which is significantly more than Israel has. It’s very good.
What does that look like in terms of population immunity? How does it compare to the 1-1/R0 threshold?
Well, 68% of the population would have a 90% effective vaccine. In addition, the FDA estimates that about 35% of the US population has been infected with SARS-CoV-2 and has about 80% immunity; let’s say that this is 40% among the unvaccinated population due to their lower propensity to take precautions. 40% of 32% is 12.8%. The end result is 68% times 90% (vaccines) plus 12.8% times 80% (natural immunity), or 71.4%.
By comparison, if R0 is 5.5, the HIT is 81.8%. If it’s 4, the HIT is 75%. So, this will leave us short of the theoretical HIT, in population immunity terms.
But it’s probably still enough. It’s more than Israel has, and they have crashed their counts. We have every reason to think, both empirically and theoretically, that if we can attain this level of vaccination, contact heterogeneity and residual precautions will be enough to push us above an effective HIT in the medium term, especially in the areas of the country that aren’t particularly prone to vaccine hesitancy.
And this is not the end of the story. It’s likely that this year, possibly this summer, COVID-19 vaccines will be approved for children as young as 6 months. When that happens the eligible population will go to nearly 100%, and if children are vaccinated at the same rate as adults, the population immunity level would rise from 71.4% to 77.7%, leaving even less room for continued transmission of COVID-19.
There is a future. We can kill the virus and end the pandemic
We have every reason to believe that if the persuadable are persuaded, the US will have something that operates like herd immunity. Cases will crash without anyone having to do anything special or onerous. New cases that arrive from abroad will fizzle inconsequentially. The pandemic will be functionally over, as regards the United States.
There will be some communities with low vaccine penetration which will suffer limited self-sustaining outbreaks for some time after the rest of the country has herd immunity. But they will be necessarily small and self-limiting, because they will fizzle out as they leave those communities, and inside them, will induce herd immunity as they continue burning. They will also convince people to vaccinate.
One scary possibility is that variants will ruin our immunity somewhat. That might happen. But it’s worth thinking through what would happen in that case.
It takes only a few months to make and trial a booster shot for a new strain, thanks to recent FDA decisions allowing boosters based on approved platforms to be approved after a Phase II trial with an immunogenicity endpoint, plus in vitro evidence of efficacy. With the majority of the population vaccinated, it will take only about one to two months to give every vaccinated person a booster. So we can have population-scale protection from a new strain in just months. And we already see that scary new variants take many months to go from first observation abroad to large outbreaks in the US; for example, the P.1 and B.1.351 variants were discovered months ago and are still months away from predominating in the US. Once we have a larger vaccinated population, a new strain will spread more slowly here, meaning we will have more time yet.
We really do have the tools in hand to end this now. We don’t need to convince the hardcore antivaxxers, and we don’t need oppressive government vaccine mandates. We just need to focus, persuade the persuadable, and vaccinate everyone who’s persuaded. The United States can win this. We can vaccinate everyone, kill the virus, and end the pandemic.
You are reporting the comment """ by on