The Pandemic is Only Beginning: The Long COVID Disaster
I just ran across this article and offer it here as food for thought:
The Pandemic is Only Beginning: The Long COVID Disaster
The ideas are still percolating in me and I’m curious to hear other people’s reactions to it.
-
Comments (17)
-
 Eric
- August 8, 2023
Eric
- August 8, 2023
Some related food for thought: This has happened before, so we have an opportunity to learn from history.
The flu pandemic of 1918-1919 was also a mass disabling event. Of course many of these newly disabled people were unable to work and were a drain on the economy. And many other people resented the burden of caring for disabled people. This was one of the key resentments that the Nazi party tapped into as they rose to power. Nazis famously targeted Jewish people, but they actually targeted disabled people first.
Takeaways:
1) Try not to become disabled.
2) Refrain from victim-shaming.
3) Study relevant historical lessons. (I’m reading “On Tyranny”, linked below.)
“On Tyranny: 20 Lessons from the 20th Century” by Timothy Snyder
My wife and I remain careful and have not had COVID yet. Well-fitted N95s help a lot with that. I also admit that I’m facing this challenge on easy mode due to working from home. Huge respect to anyone who’s pulled off the same with an in-person job.
-
Hardened
- August 18, 2023
Yes, nice to look at historical precedent. Good example, thank you.
-
Eb
- September 13, 2023
While I know #1 is serious, it did give me a little chuckle.
But seriously, if we’ve been taught anything, it’s to protect our health. Make health a priority in our lives because we only have one body. Take care of it as best you can, which means eating right, hydrating regularly, healing traumas, and moving around.
The spike protein, which can continue to replicate and accumulate in the body, is one of the main reasons why repeated infections can happen. The spike protein’s damaging effects can attack our hearts, lungs, kidneys, brains, and blood vessels.
Targeting the spike protein seems key and there’s already been studies about nattokinase, NAC, and bromelain degrading, altering, or dissolving the protein.
Sadly, I’ve had repeated infections of COVID, but since taking these on a daily basis, I have yet to be sick. Even better, I found this health remedy that conveniently has nattokinase, NAC, and bromelain all in one capsule so I’m not taking so many supplements a day because it was a lot.
Taking care of my health on a daily basis is now a priority for me.
May your health be protected as well.
Thank you for the takeaways, Eric. Very insightful.
-
-
xyz
- August 8, 2023
I work with statistical data all day, every day, so when I see an article like this it raises all kinds of red flags. Let the reader beware as the information provided in that article is misleading at best, and most definitely meant to prove the author’s overly sensational point.
-
Salvatore
- August 14, 2023
I’m the author, and would love to be wrong.
Can you be clear about how I’m being misleading? The best retorts I’ve heard so far:
- The vaccine offers better protection against long COVID than 15%. Some studies put at 20-50%. My response: Ok, maybe. Still doesn’t change my point.
- There may be some magic number of infections where long COVID stops being a risk. For example, if you’ve had 5 infections and do not have long COVID, you are unlikely to ever get it. My response: Sure, but there’s no evidence for this.
- We don’t have a good understanding of how COVID reinfections affect those with long COVID. The best data I’ve found is that survey. You can imagine a scenario where: someone contracts long COVID, recovers after 2 years, and then never gets long COVID again no matter how many times they’ve been reinfected. That would be great, but there’s no evidence for this.
- We don’t know that everyone will get COVID once a year forever. Sure, but there’s no evidence for this, and we continue to have surge after surge as the virus continues to mutate.
-
Eric
- August 14, 2023
“I’m the author, and would love to be wrong.”
Hi, Salvatore. Thanks for offering to discuss this, and welcome to The Prepared.
“A decade from now, almost one third of the world’s population could suffer from a severe chronic illness — the consequence of repeated COVID infections.”
1/3 sounds like a very high estimate.
If I were trying to estimate how many people would have long COVID 10 years in the future, I would start with how many people have it now and at some times in the past.
Your article indicates that currently about 5% of people in USA have long COVID after 3.5 years of this pandemic. If we assume prevalence increases linearly from 0% in early 2020, then we would expect 20% in 10 years. That’s already substantially less than your estimate of 33%.
But 20% is probably also high because COVID does more damage on average for the first infection than for later infections and because so many people are vaccinated now. Probably most of the current long COVID is from 2020 with slower increases since then, in which case we might expect closer to 10% in 10 years.
Do you happen to have estimates for 2021 and 2022 to give a better idea how prevalence has changed over time? That would help a lot with making a more accurate prediction.
-
xyz
- September 18, 2023
Sorry, I haven’t been following this thread. It’s generated some interesting responses. Thank you, Eric, for the detailed discussion (with graphics!).
My comments were based on your two initial assertions and your first assumption:
1. everyone on the planet will probably get COVID many times over their lifetime;
2. every time someone catches COVID there is cumulative probability that they will develop Long COVID.
3. every person catches COVID, on average, once per year going forward.
Your article implies that your chance of contracting Long COVID is based on the number of times you get COVID. You use terms like “probably”, “many times”, “cumulative probability” and “on average” but your references don’t really support your foundational assertions.
For example:
Are your conclusions based on global or US population? You start out with global population but references are primarily based on US population.
What are your constraints that bound your assumptions? At least one of the researchers in your references said their data is based on patient surveys, and subjective data isn’t as trustworthy as clinical data.
Is this really based on the number of COVID infections over your lifetime? Your references indicate that contracting Long COVID is more related to the severity of your COVID infection, both initially and subsequently. The severity of the infection is related to the patient’s overall health, and the ones with comorbidities (e.g., obesity, diabetes, heart/lung disease, etc) and especially multi-morbidities (e.g. COPD) are more likely to develop severe COVID infections than otherwise healthy individuals.
Your assumptions may be valid, but I can’t tell. If I can’t rely on them then I can’t really accept your conclusions, regardless of the math. This is unfortunate, since Long COVID is definitely real and we need to know how much it’s going to end up costing us over time.
-
Hardened
- August 18, 2023
Hi overcaffeinated, your assessment sounds potentially reassuring. Can you offer any specifics of how the article is misleading?
-
Eric
- August 19, 2023
“Hi overcaffeinated, your assessment sounds potentially reassuring. Can you offer any specifics of how the article is misleading?”
The article points to a big, important problem, and claims that it’s about 10 times bigger than it really is. This is severe exaggeration.
I was hesitant to argue against this article. Because I believe, as Salvatore does, that not nearly enough is being done to address this problem. But I also value honesty. So here’s what the data says.

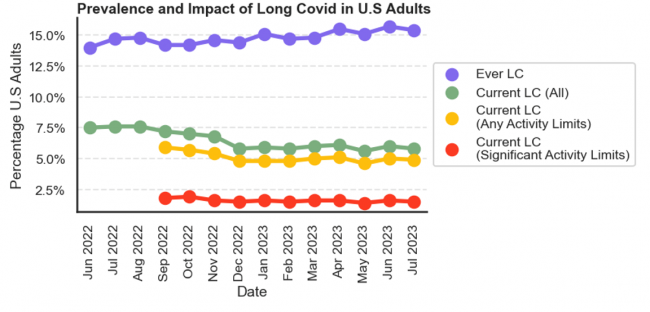
When Salvatore says that 1/3 of people will have a severe chronic illness due to long COVID, he’s saying that the red line, currently 2% and stable, is on its way up to 33%. No, it’s clearly not doing that.
Maybe Salvatore was thinking more about the purple line, people who have ever had long COVID. He does mention that long COVID is sometimes permanent. But he forgets that in most cases it is not permanent. And he forgets that in most cases the severity is not high enough to prevent people from working. He also seems not to have noticed that the purple line is also flat, having increased mostly in the first 1-2 years, and is also not likely to reach 33% in 10 years.
I encourage everyone to be careful to avoid this disease. It has caused a lot of problems and will continue to do so. For 2% of USA (6 million people), long COVID is thoroughly ruining their lives right now. The situation is likely even worse in other countries like India that had worse outbreaks. And even 2% is enough to substantially affect economies. I just refuse to look at 2% and call it 33%.
The illustration is from this article, which covers the same topic but without the exaggeration.
-
Salvatore
- August 19, 2023
Thanks Eric.
But you are not characterizing my blog accurately. In particular, this section:
Under these assumptions, after 10 years:
40% of people will have had long COVID at some point.
30% of people will have active long COVID.
7.5% of people will be so disabled from long COVID it will impact their work.To put it in terms of your chart, I’m projecting that the purple line trends up to 40%, the green line trends up to about 30%, and yellow/red line (hard to distinguish between them) trends up to about 7.5% over the next 10 years.
I would hesitate to simply take the data we have and project it linearly for several reasons:
- We don’t have that much data. Note that your yellow/red line only extend back to last September — that’s less than a year of data.
- Long COVID is challenging to define. A lot of people have it, and don’t know it. Many doctors don’t know what it is or how to diagnose it. I’ve talked to several people in their 30s now who think their brain fog is just “getting old”. Surveys of how many people in a population actually have it will be deeply flawed for this reason.
- There were restrictions in place until late 2022 in different parts of the world, limiting the number of infections/reinfections. Given that all restrictions have been lifted now, the average number of infections in the years ahead may be greater than the last 3 years.
- There is a growing body of evidence that reinfections are actually more harmful than initial infections, and may be more likely to cause long COVID than initial infections (see recent study from NIH, CDC communications about the risks of reinfection, etc.). This would actually make the situation much worse.
- The virus is continuing to mutate at a rapid pace. New variants may be more or less likely to cause long COVID. No one knows.
Lastly, I’m an analyst. My projections are, and always will be, wrong. The world is highly uncertain, and the future is unknowable. I try to take data and use it to build some type of model about what the future might look like given the path that we’re headed down. This is in the hopes that people will take this information and use it to help them make informed decisions, knowing that there’s a high degree of uncertainty no matter what. Overall, I especially wish to counter the narrative that’s being relentlessly pushed in the media and by the government that COVID is over, that COVID is a cold, that COVID can be ignored. That’s just not true.
-
Hardened
- August 30, 2023
I’ve talked to several people in their 30s now who think their brain fog is just “getting old”.
That’s horrifying!
-
Hardened
- August 19, 2023
Thanks Eric for the article and your thoughts, much appreciated. Discussions like this are why I value The Prepared community so much.
-
-
K9medic
- August 8, 2023
To be honest it is not just Covid, Post Viral Syndrome effects a lot of people. I had a bad case of flu back in the mid 1980s, caused my gums to recede, I am getting the last of my teeth extracted tomorrow and a full set of dentures.
I caught Covid over Christmas 2022. Moderate flu like symptoms for 36 hours plus complete loss of sense of smell and taste, as I was recovering, I noticed I was also having difficulty hearing family members if I was not looking directly at them. My sense of smell and taste returned slowly, but my hearing is still at the level I will need hearing aids. At the minute I am still being evaluated by the local GP surgery.
Talking to people who have not recovered their full health after Covid, some who caught it as far back as Spring 2020,
I suspect you only need to catch a virus once to suffer medical complications, though the more times you catch one the more opportunity for your body to have a bad reaction.
-
Hardened
- August 18, 2023
Yes, Long Covid is bringing awareness of Post Viral Syndrome to a lot of people including myself. I’m so sorry to hear about your difficulties with both the flu and Covid!
-
Carolyn
- August 22, 2023
Can I complain, too?
I had two, and possibly three Covid infections in 2021. One was pretty nasty. New symptoms after the last infection: Loss of appetite (I lost 55 pounds.) I was too weak to walk across the street for months; I have an autoimmune disorder that is causing my hair to fall out; I had several severe bouts of vertigo, and I still have lingering dizziness; I had acute kidney failure; and probably the most debilitating of all, my cognitive functioning cratered. I still have memory loss, aphasia, trouble sequencing things, and slow processing speed. ( I used to be a quick thinker. Now I can work 6 or 8 hours a week.)
Still, all these maladies have other, more common, causes. My doctor listens well, believes me, and is thorough and thoughtful. I feel like she is an alien that sucked me out of my car to do all kinds of high-tech testing. We have eliminated lots of scary possibilities. And the search goes on.
My hope is that as we build immunity as a population, the incidence of long covid will actually decrease.
-
Salvatore
- August 27, 2023
I’m sorry to hear that Carolyn. I hope you feel better soon.
Sadly, I don’t think we ever will build immunity as a population. Coronaviruses just don’t work that way: https://www.nature.com/articles/s41591-020-1083-1
-
Hardened
- August 30, 2023
I’m so sorry to hear about your symptoms, Carolyn!
There’s some buzz on TikTok about something called triple anticoagulant therapy including comments from Long Covid patients who have benefited from it. I don’t know anything about it but it might be worth exploring.
-
-
- Whats going on with this site - 2 months ago
- Mylar Bags - February 27, 2026
- Shot Show 2026 recap - January 22, 2026
- News for the Week 2026-1-12 - January 12, 2026
- News for the Week 2026-01-05 - January 5, 2026
This forum is heavily moderated to keep things valuable to as many people as possible. Full community policies are here. The basics:
- 1. Be nice to each other.
- 2. Stay focused on prepping.
- 3. Avoid politics, religion, and other arguments.
- 4. No unfounded conspiracies, fake news, etc.
- 5. Debate ideas, not people.